Verified By IT Certified Experts
CertsTopics.com Certified Safe Files
Up-To-Date Exam Study Material
99.5% High Success Pass Rate
100% Accurate Answers
Instant Downloads
Exam Questions And Answers PDF
Try Demo Before You Buy

A 47-year-old man presented with a 2-month history of polyuria and polydipsia. He awoke six times most nights to pass copious volumes of urine despite not drinking any fluid for 4 hours before going to bed.
Investigations:
MR scan of pituitary fossasee image
A water deprivation test confirmed the diagnosis of cranial diabetes insipidus.
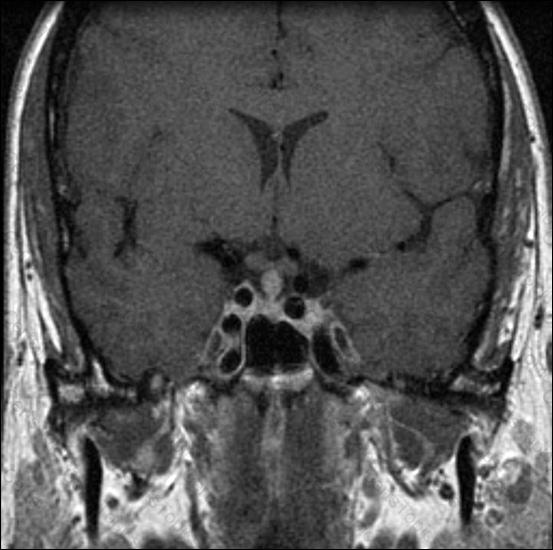
What is the most likely underlying diagnosis?
A 55-year-old woman presented with thirst, polyuria and polydipsia. Her symptoms had started 9 months previously following a road traffic accident. Her past medical history was normal and she was not taking any regular medication.
On examination, her blood pressure was 130/80 mmHg with no postural drop. Urine volume measured 5 L in 24 hours.
Investigations:
serum sodium131 mmol/L (137–144)
serum potassium3.6 mmol/L (3.5–4.9)
serum urea2.0 mmol/L (2.5–7.0)
serum corrected calcium2.40 mmol/L (2.20–2.60)
fasting plasma glucose6.4 mmol/L (3.0–6.0)
serum osmolality278 mosmol/kg (278–300)
urinary osmolality100 mosmol/kg (100–1000)
What is the most likely diagnosis?
A 17-year-old Caucasian girl presented with primary amenorrhea.
On examination, her body mass index was 21 kg/m2 (18–25). Her body habitus was normal and she had appropriate breast development. There was no hirsutism or acne.
Investigations:
serum oestradiol<180 pmol/L (200–400)
serum testosterone31.7 nmol/L (0.5–3.0)
serum follicle-stimulating hormone4.0 U/L (2.5–10.0)
serum luteinising hormone6.0 U/L (2.5–10.0)
What is the most likely diagnosis?
Copyright © 2021-2025 CertsTopics. All Rights Reserved
