A 67-year-old man underwent an isotope bone scan after being found to have a raised serum alkaline phosphatase (of bone origin). The blood test had been ordered because of mild lower back pain, which had now resolved. He was not taking any medication.
Examination was normal.
Investigations:
isotope bone scansee image
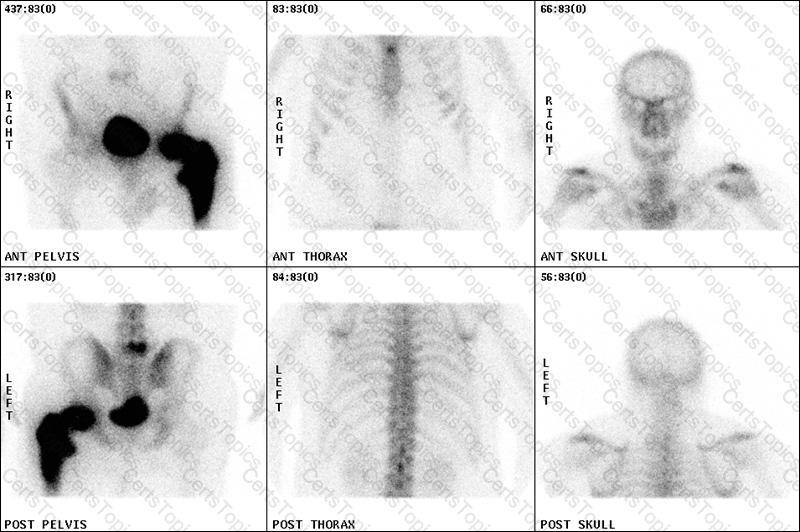
What is the most likely diagnosis?
A 73-year-old man with type 2 diabetes mellitus was reviewed because of deteriorating blood glucose control. He was taking metformin 850 mg twice daily.
On examination, his body mass index was 29 kg/m2 (18–25).
Investigations:
serum creatinine102 µmol/L (60–110)
haemoglobin A1c66 mmol/mol (20–42)
According to the NICE guidelines (CG87, May 2009), what would be the most appropriate additional treatment?
A 48-year-old woman presented with a 2-year history of weight gain, easy bruising and mood disturbance.
Investigations:
fasting plasma glucose6.9 mmol/L (3.0–6.0)
low-dose dexamethasone suppression test (2 mg/day for 48 h):
serum cortisol200 nmol/L (<50)
24-h urinary free cortisol (?3)670, 400 and 300 nmol (55–250)
plasma adrenocorticotropic hormone (09.00 h)25.0 pmol/L (3.3–15.4)
MR scan of pituitarynormal
What test is most likely to give a definitive diagnosis?
A 55-year-old woman presented with a 3-week history of nausea and vomiting. Her only medical complaints were frequent dyspepsia, for which she was taking indigestion tablets, and asthma for which she was taking a salbutamol inhaler as required.
On examination, there was no evidence of lymphadenopathy, her chest was clear on auscultation and abdominal examination was normal.
Investigations (before and after taking omeprazole for 3 weeks):
beforeafternormal
erythrocyte sedimentation rate (mm/1st h)44<30
serum creatinine (µmol/L)17011060–110
serum corrected calcium (mmol/L)2.852.402.20–2.60
serum phosphate (mmol/L)1.90.8–1.4
serum angiotensin-converting enzyme (U/L)8525–82
plasma parathyroid hormone (pmol/L)0.44.40.9–5.4
What is the most likely cause of the hypercalcaemia?
Copyright © 2021-2025 CertsTopics. All Rights Reserved
